🩺 Medical Editor’s Note (2026 Verified Data)
This technical guide has been verified against 2026 medical tourism standards in Turkey.
Verified Price Range: Gastric Sleeve: 3,500 – 5,500 USD | Gastric Bypass: 4,500 – 7,500 USD | Gastric Balloon: 2,000 – 3,000 USD
Facility Standards: JCI Accredited, Ministry of Health Regulated.
Currency: USD / EUR / GBP accepted at all clinics.
Gastric Bypass vs. Gastric Sleeve for Acid Reflux (GERD): Making the Right Choice
Understanding the Impact of Bariatric Surgery on Gastroesophageal Reflux Disease (GERD)
Gastroesophageal Reflux Disease (GERD), commonly experienced as heartburn and acid indigestion, affects a significant portion of the population. While often manageable with lifestyle modifications and pharmacological interventions, GERD can become debilitating and, critically, may be *exacerbated* or, in certain cases, *resolved* by bariatric surgery. For patients considering weight loss surgery who also suffer from GERD, the choice between Gastric Bypass and Gastric Sleeve procedures demands a nuanced understanding of their differing physiological effects on the lower esophageal sphincter (LES) and gastric acid production. This pillar focuses on the ‘what’ and ‘why’ of this complex interplay, grounding our discussion in medical foundation and global standards.
The Pathophysiology of GERD and Bariatric Surgery’s Influence
GERD arises from a compromised barrier between the stomach and the esophagus. This barrier comprises the LES, a ring of muscle that normally remains contracted to prevent gastric contents from flowing backwards (refluxing). When the LES weakens or relaxes inappropriately – often due to factors like obesity, hiatal hernia, or increased intra-abdominal pressure – acid and pepsin can irritate the esophageal lining, causing inflammation (esophagitis) and characteristic GERD symptoms. Bariatric surgery, by inducing significant weight loss and altering gastrointestinal physiology, directly impacts these contributing factors.
Importantly, the impact differs substantially between Gastric Bypass and Gastric Sleeve. The Gastric Bypass, or Roux-en-Y Gastric Bypass (RYGB), involves creating a small stomach pouch and connecting it directly to the jejunum, bypassing a significant portion of the duodenum and stomach. This alteration has profound effects on both mechanical and hormonal regulation of GERD. The bypassed stomach produces less ghrelin (the “hunger hormone”), which can indirectly reduce LES relaxations. More significantly, the RYGB creates a functional “buffer” against reflux. The newly created Roux limb acts as a biological anti-reflux mechanism; gastric contents are directed away from the LES, reducing the frequency and severity of reflux episodes. However, this isn’t a guaranteed outcome. A leak at the anastomosis (connection point) is a serious post-operative complication that could *cause* or worsen reflux, though modern surgical techniques and meticulous attention to detail minimize this risk.
Gastric Sleeve: A More Complex Relationship with GERD
The Gastric Sleeve (Vertical Sleeve Gastrectomy – VSG) involves removing approximately 80% of the stomach, creating a narrow, tubular “sleeve.” While effective for weight loss, the VSG’s impact on GERD is more variable and often unpredictable. The removal of the stomach’s outer fundus, a critical reservoir for gastric distention, reduces the ability to accommodate large volumes of food. This can reduce the incidence of transient LES relaxations triggered by gastric distention. However, VSG also *increases* the intra-abdominal pressure due to the anatomical changes. This increased pressure can, paradoxically, worsen GERD in some patients.
A key consideration is pre-operative GERD severity. Patients with pre-existing, severe GERD are generally not considered ideal candidates for VSG. The surgery can exacerbate their symptoms, leading to persistent esophagitis and potential Barrett’s esophagus (a precancerous condition). Preoperative evaluation, including 24-hour pH monitoring and esophagography, is crucial to assess the extent of reflux and guide surgical decision-making. In patients with mild to moderate GERD, the VSG may offer some improvement, but the risk of worsening symptoms must be carefully weighed. A newer technique, the magnetic sphincter banding (LINX) procedure, can sometimes be considered concurrently with VSG in select patients with mild GERD to reinforce the LES.
Surgical Technique & its Correlation to GERD Outcomes
The technical execution of both procedures significantly impacts GERD outcomes. In RYGB, the length of the Roux limb and the tension at the gastrojejunostomy (the connection between the gastric pouch and jejunum) are critical. A longer Roux limb offers greater anti-reflux protection but may increase the risk of dumping syndrome. In VSG, the angle at which the gastric sleeve is created and the complete removal of the fundus are vital for optimizing outcomes and minimizing post-operative complications. Surgeons specializing in bariatric surgery and experienced in managing GERD are crucial for optimal results.
Global Standards and Cost Considerations for Bariatric Surgery
CureHoliday.com prioritizes patient safety and adheres to the highest global standards. For procedures performed internationally, particularly in Turkey, we partner with facilities accredited by JCI (Joint Commission International) and regulated by the Turkish Ministry of Health, ensuring adherence to rigorous quality control measures.
Here’s a breakdown of approximate costs (as of late 2023):
- Gastric Sleeve: 3,500 – 5,500 USD
- Gastric Bypass: 4,500 – 7,500 USD
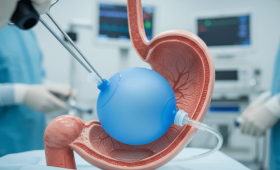
- Gastric Balloon: 2,000 – 3,000 USD (Note: Gastric Balloon is not a primary solution for GERD and is generally not performed in conjunction with GERD management.)
Currency fluctuations can affect pricing, with options available in USD, EUR, and GBP. All patients travelling to Turkey are eligible for an E-visa for stays up to 90 days. We offer recovery hubs in diverse locations including Istanbul (City/Boutique hotels), Antalya (Resort/Beach access), and Izmir (Aegean/Thermal resorts) to cater to individual preferences.
Patient Selection Criteria & BMI Considerations
Regardless of the chosen procedure, adherence to established criteria is paramount. Generally, candidates for bariatric surgery must have a Body Mass Index (BMI) greater than 35, or a BMI greater than 30 with significant co-morbidities (such as type 2 diabetes, hypertension, sleep apnea). Comprehensive pre-operative evaluation, including a thorough medical history, physical examination, psychological assessment, and diagnostic testing (including upper endoscopy and pH monitoring for GERD patients), is essential to determine surgical suitability and optimize outcomes.
It’s crucial to remember that bariatric surgery is not a ‘cure’ for GERD, but a potentially modifying intervention. Patient education and realistic expectations are vital components of a successful outcome.
Gastric Bypass vs. Gastric Sleeve for Acid Reflux (GERD): The Surgical Journey
For patients suffering from severe Gastroesophageal Reflux Disease (GERD) alongside obesity, bariatric surgery offers a potentially life-changing solution. However, choosing between Roux-en-Y Gastric Bypass (RYGB) and Sleeve Gastrectomy (SG) requires careful consideration, particularly regarding its impact on GERD symptoms. This pillar delves into the technical aspects of each procedure, explores a representative patient case, and outlines strategies for mitigating potential risks, focusing on the patient experience through CureHoliday.
Technical Details: Gastric Bypass (RYGB)
RYGB is considered the ‘gold standard’ bariatric procedure due to its demonstrated long-term efficacy in weight loss and resolution of co-morbidities. The surgery involves creating a small stomach pouch (approximately 30ml) and connecting it directly to the jejunum, bypassing a significant portion of the stomach and duodenum. This altered anatomy achieves weight loss through several mechanisms:
- Restriction: The smaller stomach pouch limits food intake.
- Malabsorption: Bypassing the duodenum reduces caloric and nutrient absorption.
- Hormonal Changes: RYGB significantly alters gut hormone secretion, impacting appetite, satiety, and glucose metabolism. Specifically, it impacts GLP-1 and PYY, which play key roles in appetite suppression.
From a GERD perspective, RYGB often *resolves* or significantly *improves* symptoms. The bypassed duodenum produces gastric inhibitory peptide (GIP), and removing its influence on the stomach can reduce acid production. Moreover, the weight loss itself reduces intra-abdominal pressure, further alleviating reflux. However, a small percentage (estimated 5-15%) experience de novo GERD post-operatively, often related to pouch distension or hiatal hernia formation. This risk is higher in patients with pre-existing large hiatal hernias which should be addressed during the surgery.
The typical operative time is 60-90 minutes, often performed laparoscopically. Post-operative care involves a staged diet progression, starting with liquids and gradually advancing to purees, soft foods, and finally, solid foods. Vitamin and mineral supplementation (B12, iron, calcium, vitamin D) is crucial for life-long adherence due to malabsorption.
Technical Details: Gastric Sleeve (SG)
SG involves removing approximately 80% of the stomach, leaving a narrow, tube-shaped stomach (the ‘sleeve’). This restricts food intake and reduces ghrelin, the ‘hunger hormone’. While primarily restrictive, SG also induces some hormonal changes, though to a lesser extent than RYGB.
Unlike RYGB, SG can sometimes worsen pre-existing GERD, or even induce it in patients without prior symptoms. The reduced stomach capacity can increase intra-abdominal pressure, and the loss of the lower esophageal sphincter (LES) support provided by the removed gastric fundus can exacerbate reflux. The incidence of post-operative GERD with SG is estimated at 15-30%. Careful patient selection, particularly excluding those with significant pre-existing GERD or large hiatal hernias, is paramount. Pre-operative pH monitoring (24-hour impedance-pH testing) is often recommended.
Sleeve gastrectomy generally takes 45-60 minutes laparoscopically. Post-operative diet progression is similar to RYGB, but patients may experience nausea and vomiting more frequently initially due to the narrow gastric sleeve. Vitamin supplementation (B12, iron, vitamin D) is also necessary, though malabsorption is less pronounced than with RYGB.
Persona Case Study: Eleanor Davies, 45, UK
Eleanor, a 45-year-old librarian from the UK, presented with a BMI of 41 and longstanding, debilitating GERD resistant to proton pump inhibitors (PPIs). She also had type 2 diabetes and hypertension. Pre-operative investigations revealed a small hiatal hernia (<2cm). After thorough consultation with the CureHoliday surgical team, and comprehensive assessments – including upper endoscopy, manometry, and 24-hour pH monitoring – a decision was made to proceed with RYGB.
Eleanor elected for surgery in Istanbul, benefiting from the JCI-accredited facilities and the package which included pre-op assessments, surgery, hospital stay (7 days), post-op care, and hotel accommodation. Her CureHoliday care coordinator assisted with visa requirements (E-visa) and airport transfers. The surgery was performed without complication. Eleanor adhered to the prescribed diet progression and experienced significant improvement in her GERD symptoms within 4 weeks. Her diabetes was well-controlled, and she lost 65kg in the first 18 months post-surgery. She continues to receive dietary and lifestyle guidance from the CureHoliday team.
Risk Mitigation: Surgical & Post-Operative
Minimizing risks is central to CureHoliday’s patient-centric approach. For both procedures, the following strategies are employed:
- Pre-operative Optimization: Addressing co-morbidities, optimizing nutrition, and cessation of smoking are essential. Patients with pre-existing GERD undergo thorough evaluation to assess the severity and suitability for each procedure.
- Surgical Technique: Experienced bariatric surgeons utilize meticulous laparoscopic techniques to minimize blood loss, infection risk, and post-operative adhesions. In cases with hiatal hernias, a concurrent repair is performed.
- Anastomosis Quality (RYGB): Ensuring a leak-proof anastomosis (connection between the stomach pouch and jejunum) is critical. Intraoperative leak testing (e.g., using air or saline) and careful surgical technique are employed.
- Post-operative Monitoring: Close monitoring for complications such as leaks, bleeding, infection, and venous thromboembolism.
- Dietary Counseling: A registered dietitian provides individualized dietary guidance to ensure adequate nutrition, prevent deficiencies, and manage potential dumping syndrome (RYGB).
- Proton Pump Inhibitor (PPI) Therapy: While RYGB often reduces PPI needs, continued use may be recommended in some cases, particularly post-SG, to manage residual or new-onset GERD.
- Long-Term Follow-up: Regular follow-up appointments (virtual or in-person) with the surgical team and dietitian to monitor progress, address concerns, and ensure long-term health.
CureHoliday prioritizes patient safety through careful surgeon selection, adhering to strict Turkey medical standards (JCI accreditation and Ministry of Health regulations), and providing comprehensive pre- and post-operative care. The total cost of a gastric sleeve is approximately 3,500 – 5,500 USD, while a gastric bypass ranges from 4,500 – 7,500 USD. A gastric balloon, considered a less invasive option, costs approximately 2,000 – 3,000 USD but is not suitable for all patients, and has lower long-term efficacy.
For UK, US, and EU citizens, CureHoliday assists with travel arrangements including E-visa applications allowing for a 90-day stay. Patients can choose from recovery options in Istanbul (City/Boutique), Antalya (Resort/Beach) or Izmir (Aegean/Thermal) depending on their preference.
Navigating Post-Operative Recovery: A Comparative Analysis of Gastric Bypass & Gastric Sleeve
Following bariatric surgery – whether a Roux-en-Y Gastric Bypass (RYGB) or a Sleeve Gastrectomy (SG) – a robust and meticulously planned recovery phase is paramount to achieving sustained weight loss and resolving co-morbidities like Gastroesophageal Reflux Disease (GERD). This pillar will delve into the logistical nuances of recovery for both procedures, with a specific focus on the emerging landscape of medical tourism in Turkey (Antalya and Istanbul) and a detailed 2026 cost analysis compared to Western healthcare systems. We will analyze the subtle, yet critical, differences in the recovery trajectory post-surgery, especially concerning GERD resolution, and provide practical guidance for patients.
Early Post-Operative Phase (0-30 Days): Hospital Stay & Initial Management
The immediate post-operative period, typically spanning 1-3 days for both RYGB and SG in Turkish facilities, focuses on pain management, wound care, and initiating a liquid diet. However, subtle differences emerge. RYGB patients require closer monitoring for ‘dumping syndrome’ – a rapid gastric emptying that can cause nausea, dizziness, and diarrhea – necessitating stringent dietary adherence and potential pharmacologic intervention with octreotide in severe cases. SG patients, while less prone to dumping, require careful evaluation for ‘staple line leaks’, although advancements in surgical techniques and reinforcement methods have significantly reduced this risk.
In both cases, early ambulation is crucial. This isn’t merely about preventing deep vein thrombosis (DVT), but also stimulating peristalsis – the wave-like muscle contractions that move food through the digestive tract. Post-operative ileus, a temporary cessation of intestinal motility, is more common after RYGB due to the bowel rearrangement. This necessitates nasogastric (NG) tube management in some instances to decompress the stomach. Modern protocols prioritize Enhanced Recovery After Surgery (ERAS) pathways, emphasizing multimodal analgesia (opioid-sparing pain control), early oral intake of clear fluids, and proactive management of potential complications.
Intermediate Recovery (30-90 Days): Dietary Progression & Lifestyle Adaptation
This phase sees a gradual transition from liquids to pureed foods, then to soft solids, and finally to a regular, albeit modified, diet. The dietary progression differs significantly between the two procedures. RYGB patients are permanently restricted in portion size and require a highly structured eating pattern, emphasizing protein intake and vitamin/mineral supplementation (specifically B12, iron, calcium, and vitamin D) due to impaired absorption. SG patients, while also requiring portion control, have a larger functional stomach volume and generally exhibit fewer micronutrient deficiencies, though monitoring is still essential.
Crucially, the impact on pre-existing GERD diverges. While both procedures can *improve* GERD symptoms by reducing intra-abdominal pressure and overall weight, RYGB has a statistically significant advantage. The bypassed duodenum and the creation of a smaller gastric pouch reduce the amount of acid refluxing into the esophagus. However, a subset of RYGB patients experience ‘alkaline reflux’ – bile reflux – which can be more challenging to manage than traditional acid reflux. SG, while not as potent in resolving GERD, often provides sufficient relief, and the risk of alkaline reflux is lower. Pre-operative esophageal manometry and 24-hour pH impedance testing are vital to predict individual responses and guide surgical selection.
Long-Term Recovery & Maintenance (90+ Days): Addressing Complications & Sustaining Results
Long-term follow-up is vital for both procedures. RYGB patients require lifelong monitoring for nutritional deficiencies, bowel obstructions (adhesions are a possibility with any abdominal surgery), and marginal ulceration. SG patients require monitoring for strictures (narrowing of the gastric sleeve) and long-term weight regain.
A frequently overlooked aspect is the psychological recovery. Bariatric surgery induces significant physiological and lifestyle changes, and patients often benefit from ongoing support groups, nutritional counseling, and even psychological therapy to address body image issues and maintain healthy coping mechanisms.
Turkey as a Destination for Bariatric Surgery: Cost & Logistics (2026 Projections)
The burgeoning medical tourism industry in Turkey, particularly in Istanbul and Antalya, offers compelling cost advantages. Current estimates for a Gastric Sleeve range from 3,500 – 5,500 USD, while Gastric Bypass falls within the 4,500 – 7,500 USD range. A Gastric Balloon procedure is available for lower BMI patients at 2,000 – 3,000 USD. We anticipate a moderate increase in these costs by 2026 (estimated 5-10% inflation), but Turkey is still projected to remain significantly more affordable than equivalent procedures in the US, Canada, and most Western European nations.
However, cost isn’t the sole determining factor. The quality of care is paramount. Reputable Turkish facilities adhere to stringent JCI (Joint Commission International) Accreditation and are regulated by the Ministry of Health. Patients should meticulously vet their chosen hospital and surgeon, verifying credentials and experience.
- Istanbul: Offers a vibrant city experience with numerous accredited hospitals and a wide range of accommodation options, from luxury hotels to boutique guesthouses.
- Antalya: Provides a resort-style recovery environment with beach access, facilitating gentle rehabilitation and relaxation.
- Izmir: Known for its thermal spas and Aegean coastline, offering a unique recovery experience focused on wellness and rejuvenation.
The logistical considerations are also crucial. Most UK/US/EU citizens can obtain an E-visa for a 90-day stay in Turkey. Accommodation, transportation, and post-operative care can be bundled into comprehensive packages offered by medical tourism agencies. Currency exchange rates are favorable, with pricing typically offered in USD, EUR, and GBP.
Addressing GERD Specifically: A Post-Surgical Regimen
Regardless of the chosen procedure, a long-term GERD management plan is critical. This includes:
- Dietary Modification: Avoiding trigger foods (caffeine, alcohol, chocolate, spicy foods, fatty foods), eating smaller, more frequent meals, and maintaining adequate hydration.
- Lifestyle Adjustments: Elevating the head of the bed, avoiding late-night eating, and maintaining a healthy weight.
- Pharmacological Management: For persistent symptoms, proton pump inhibitors (PPIs) or H2 receptor antagonists may be necessary, although the goal is to minimize long-term reliance on medication.
- Endoscopic Surveillance: Periodic endoscopies may be recommended to monitor the esophagus and detect any complications.
Patients with persistent or worsening GERD symptoms post-surgery should consult their surgeon or a gastroenterologist for further evaluation and management. The requirement for surgery remains a BMI > 35 or > 30 with co-morbidities.
Ready to consult a specialist? Schedule a Free Consultation for Gastric Bypass vs. Gastric Sleeve for Acid Reflux (GERD) in Turkey with cureholiday.com